Oral Surgery
Types of Dental Bone Grafts: Autograft, Allograft, Xenograft, and Synthetic
The four bone-graft materials in dentistry: what each is, where it's from, and how to choose, with guidance for religious, ethical, or vegan concerns.
Written by Dr. Husna Khan, DDS
Serenity Dental of Bloomingdale · April 29, 2026
Educational purposes only. Material choice should be discussed at consultation. Call (630) 359-0105.
There is a moment in many implant consultations when the patient asks where the graft material comes from. The answer can range from “your own bone” to “donor tissue” to “processed cow bone” to “fully synthetic ceramic.” All four are routine in modern dentistry. All four work. The differences matter for some patients more than others — particularly for those with religious, ethical, or vegan concerns about the source.
This guide walks through each of the four bone graft categories, what each is, when each is recommended, and how to choose.
The four categories at a glance
Bone graft types
| Type | Source | Common use | Notes |
|---|---|---|---|
| Autograft | Patient’s own bone | Largest defects | Best healing; second surgical site |
| Allograft | Human donor (cadaveric) | Most common | Processed and sterile |
| Xenograft | Animal source (typically bovine) | Sinus lift, ridge | Slower remodeling, predictable scaffold |
| Alloplast | Synthetic (calcium phosphate, etc.) | Smaller defects | Fully synthetic; no disease risk |
Bone graft material categories

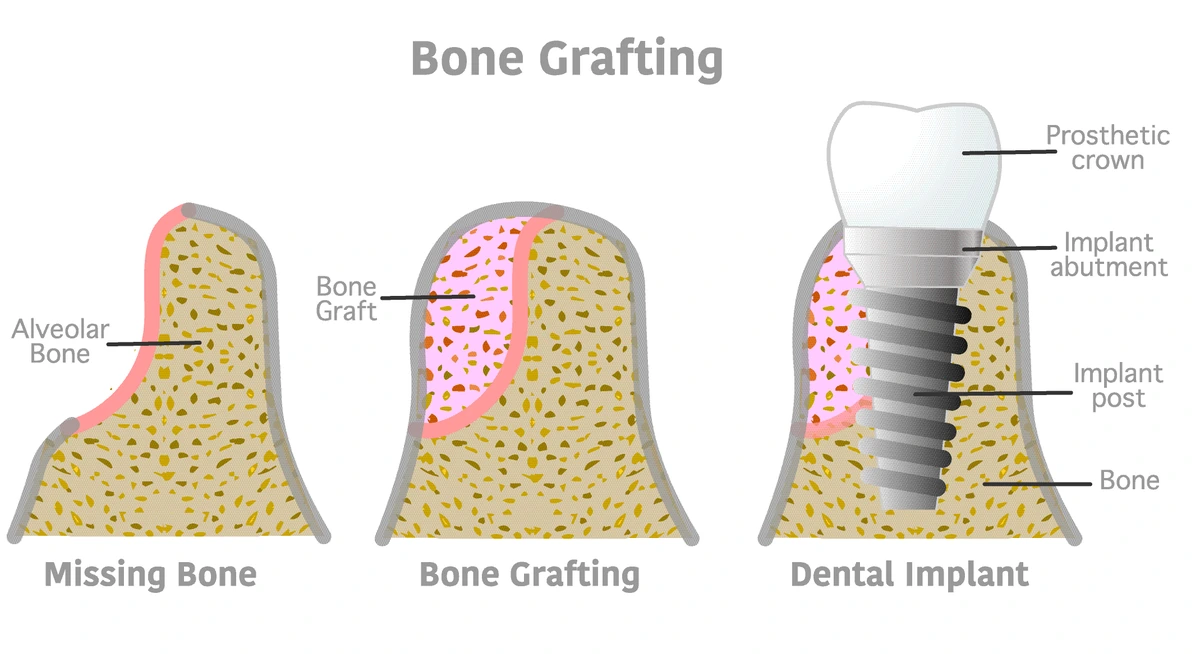
The four categories — autograft, allograft, xenograft, and alloplast — describe where the bone material came from. The biology of how each integrates with the patient’s own bone is similar across all four: the graft acts as a scaffold, the patient’s own bone-forming cells migrate in, and over 3 to 6 months the scaffold is gradually replaced by living native bone.
Autograft — your own bone
Autograft is bone harvested from another part of the patient’s own body and transplanted into the dental site. Common harvest locations include the chin (the symphysis), the area behind the lower wisdom tooth (the ramus), and in larger reconstructions the hip.
This was the first bone grafting approach used in dentistry. It is sometimes called the gold standard because the bone contains living osteoblasts — the cells that actively form new bone — and there is zero risk of immune reaction since it is the patient’s own tissue.
The downside is the second surgical site. Harvesting bone from the chin, for example, requires its own incision, healing period, and post-operative care. For routine single-implant cases, the trade-off rarely makes sense. Autograft is usually reserved for large reconstructive cases where the volume of bone needed exceeds what donor or synthetic materials can predictably support, or where a critical case demands the fastest possible integration.
Allograft — processed donor bone
Allograft is bone from a deceased human donor. The phrase “cadaver bone” appears in some patient questions, and the technical answer is yes — allograft tissue comes from donors. What that phrase tends to undersell is how thoroughly the material is processed before it ever reaches a dental office.
Tissue is harvested at American Association of Tissue Banks (AATB) accredited tissue banks. Donors are screened for infectious disease against the same standards used for organ donation. The bone is then sterilized, decellularized, demineralized in some preparations, freeze-dried, and packaged in single-use vials. By the time the material is placed in the patient’s mouth, it contains no living cells — only the mineral and collagen scaffold structure.
This processing matters: there has never been a documented case of disease transmission from a properly processed FDA-cleared dental allograft. The American Academy of Periodontology and the AAOMS both endorse allograft as a standard, safe option for routine grafting.
For most single-implant cases at our office, allograft is the workhorse material. It eliminates a second surgical site, integrates predictably, and has decades of clinical track record.
Patients who feel uncomfortable with donor tissue for personal, religious, or ethical reasons should say so. Synthetic alternatives exist and work well — there is no clinical reason to choose allograft over alloplast against the patient’s preference.
Xenograft — processed animal bone
Xenograft is bone from a non-human animal source, almost always bovine (cow). The brand most patients have heard of is Bio-Oss, manufactured by Geistlich. Other brands exist; the underlying material is similar.
Cow bone is used because the mineral structure of the bovine skeleton is remarkably similar to human bone. After processing, all organic material — proteins, fats, cells — is removed. What remains is the inorganic mineral framework, primarily hydroxyapatite. The final product is essentially a porous ceramic scaffold of bovine origin.
Xenograft is particularly common in sinus lifts because the material resorbs slowly. That slow resorption is an advantage in the sinus, where graft volume needs to hold its shape under the elevated sinus membrane while new bone forms around it.
Xenograft has the same patient considerations as allograft. Patients who prefer to avoid animal tissue for vegan, religious, or ethical reasons should request a synthetic alternative. The clinical outcomes for routine implant grafting are equivalent.
Alloplast — fully synthetic graft
Alloplastic graft material is manufactured in a laboratory. No human or animal source. The most common formulations are:
- Beta-tricalcium phosphate (β-TCP) — a calcium-phosphate ceramic that resorbs as new bone replaces it. Often used in socket preservation.
- Hydroxyapatite (HA) — chemically similar to the mineral component of natural bone, but slower to resorb. Sometimes blended with β-TCP for a balance of stability and turnover.
- Bioactive glass — silica-based ceramics that release calcium and phosphate ions to encourage local bone formation.
Alloplast was developed in part to give clinicians and patients an option with no biological source. The material has improved substantially in the last fifteen years. Modern alloplast graft outcomes for routine single-implant cases are clinically equivalent to allograft and xenograft in most published comparisons.
Alloplast is the answer for patients who:
- Follow a strict vegan lifestyle
- Hold religious or cultural beliefs that preclude using human or animal donor tissue
- Have concerns about donor tissue despite the safety record
- Want the simplest source story possible: a manufactured ceramic, nothing more
In our office, when a patient mentions any of these preferences, the conversation shifts to a synthetic option without any change in the clinical plan or success expectation.
Combination grafts
In practice, single-material grafts are common but combination grafts are also routine. A surgeon may mix allograft and synthetic alloplast to balance scaffold stability with quicker resorption. A xenograft may be combined with the patient’s own bone particles harvested from the surgical site itself.
The ratios are case-dependent and rarely something the patient needs to weigh in on. What matters at the consultation is whether the patient has a preference about source material — donor versus animal versus synthetic — so the case plan can be built around that preference.
How should you think about choosing?
For most patients, the choice is best framed two ways.
Clinically. Most single-implant cases work well with allograft, xenograft, or alloplast. Autograft is reserved for large reconstructions. The clinician picks based on case complexity, sinus involvement, and patient health factors.
Personally. If the patient cares about source material — religious, ethical, vegan, personal preference — that overrides the clinician’s default. A synthetic alloplast is available, works well, and there is no reason to choose otherwise against the patient’s wishes.
The conversation should happen at consultation, before the day of surgery. In our office, we ask every grafting patient at consult whether they have a source preference. Roughly one in twenty patients does, and we adjust the plan accordingly with no change in expected outcome.
A note on safety
All four categories carry FDA clearance. All four have decades of clinical track record. Documented disease transmission from a properly processed FDA-cleared dental graft has not occurred. The Cochrane Oral Health database has reviewed implant outcomes across graft material types and reported broadly comparable success rates for routine single-implant cases.
What matters for safety in any individual case is the surgical technique, the post-operative care, the patient’s overall health, and most of all whether the patient avoids smoking during healing. Material choice is rarely the limiting factor.
Bottom line
Four bone graft material categories are used in modern dentistry. Autograft is the patient’s own bone. Allograft is processed human donor tissue. Xenograft is processed animal bone, almost always bovine. Alloplast is fully synthetic. All four work. For routine single-implant cases the choice is shaped more by patient preference than by any meaningful clinical difference.
To discuss the right material for your case — including non-animal and non-donor options — call Serenity Dental in Bloomingdale at (630) 359-0105. Related: bone grafting service page · what is a dental bone graft.
Common questions about graft material types
What are the four types of dental bone grafts?
Is a dental bone graft cadaver bone?
What is the safest type of dental bone graft?
Are there vegan or animal-free dental bone graft options?
Is xenograft made from cow bone?
Which bone graft material does Serenity Dental use?
Does graft material type affect healing time?
Educational content only. Recommendations are personalized after an exam and any needed imaging.
About this article
Educational purposes only. Material classifications follow AAOMS clinical categorization of bone graft sources. Tissue bank standards reflect American Association of Tissue Banks (AATB) accreditation. The Cochrane Oral Health database has reviewed comparative outcomes across graft material types in single-implant grafting. Material choice for any individual patient should be made at consultation.
.
Need help with this in real life?
Reading helps. Talking to someone who can look at your actual teeth and symptoms helps more. If you want a clear next step, we’re here.
Related articles
What Is a Dental Bone Graft? A Complete Patient Guide
A dental bone graft rebuilds jawbone where a tooth was lost. What it is, when it's needed, why bone disappears, and how it restores volume for an implant.
Read article →Broken Tooth Extraction: What to Expect
How broken tooth extraction differs from simple extraction -- surgical approach, cost, recovery, and whether a regular dentist can remove a broken tooth.
Read article →Infected Tooth Extraction: When It's Needed and What to Expect
When an infected tooth needs extraction vs saving, antibiotics before extraction, post-op infection signs, and what recovery looks like.
Read article →