Preventive Dentistry
What Is a Dental Sealant? A Plain-English Guide
A dental sealant is a thin protective coating on a back-tooth chewing surface. What sealants are made of, how they prevent cavities, and who needs them.
A dental sealant is a thin protective coating applied to the chewing surface of a back tooth to prevent cavities from forming in the deep grooves where toothbrush bristles cannot reach. That is the entire concept. The procedure takes minutes per tooth, requires no drilling and no anaesthetic, and the protection lasts five to ten years. The CDC, ADA, and AAPD all recommend sealants as a first-line preventive intervention for school-age children, and adults with deep groove anatomy qualify too.
Written by Dr. Husna Khan, DDS
Serenity Dental of Bloomingdale · April 27, 2026
Educational purposes only. Sealant candidacy depends on each patient’s groove anatomy, cavity history, and exam findings. Call (630) 359-0105 to discuss specifics for your situation.
The simplest possible explanation
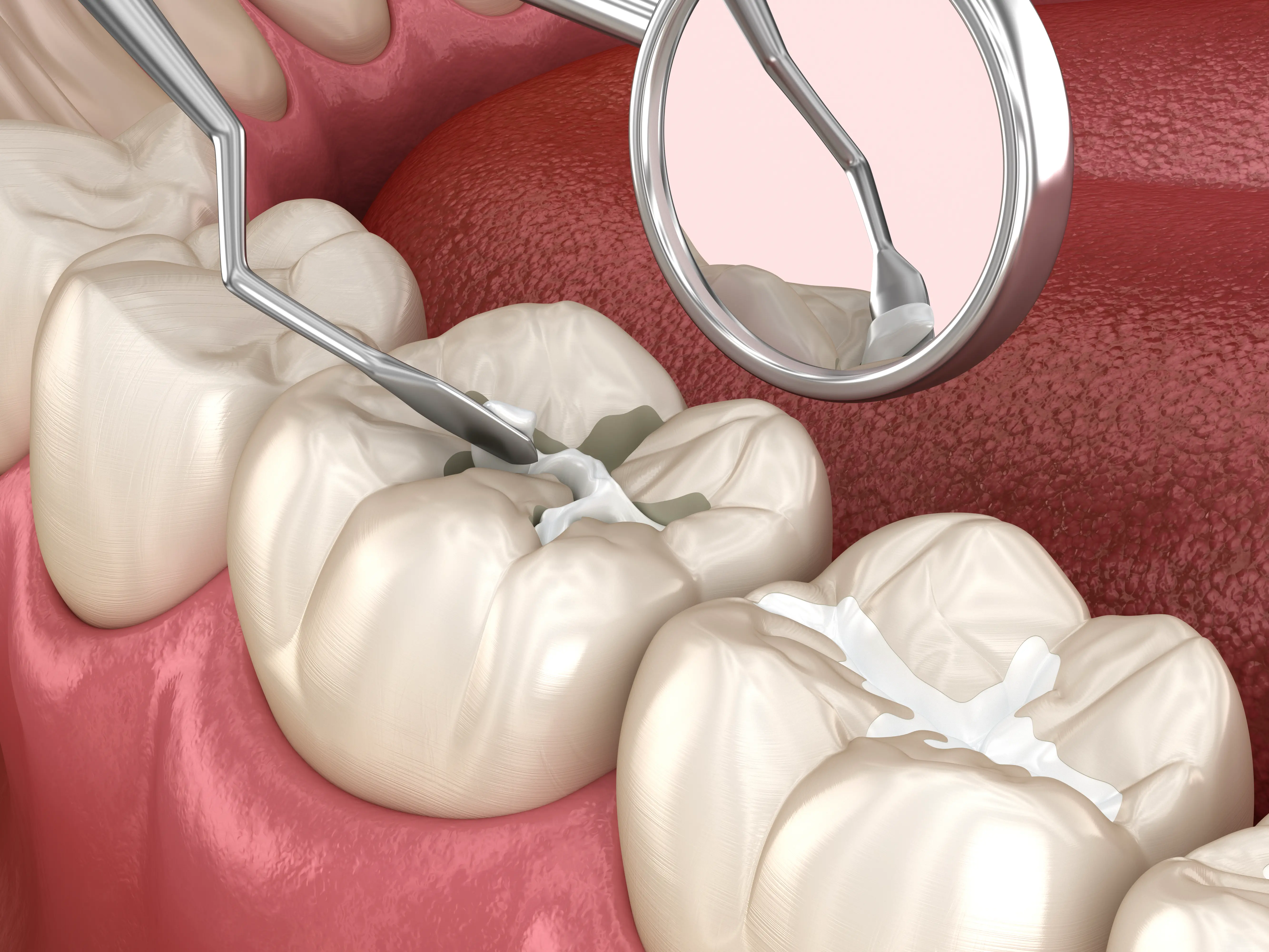
Picture a molar from above. The chewing surface has small hills and valleys — the cusps that grind food and the deep grooves between them. Those grooves are called pit-and-fissure anatomy. They are deeper than they look. Many fissures run deep enough that a single toothbrush bristle cannot fit to the bottom, no matter how carefully a child or adult brushes.
That is where almost all childhood cavities start.
A sealant is a liquid resin that flows into those grooves, bonds to the enamel, and cures into a smooth surface. After placement, the tooth no longer has a deep groove for bacteria to settle in. The toothbrush can finally clean the entire chewing surface effectively. The cavity that would have formed in that groove never starts.
What are sealants made of?
Resin-based sealants
The most common type. Bis-GMA resin matrix with filler particles, similar to tooth-coloured composite filling material. Cures with a blue light in seconds.
Used for most routine sealants on dry isolation-friendly teeth.
Glass ionomer sealants
Alternative material that releases small amounts of fluoride over time. Bonds in slightly moist conditions when full isolation is difficult.
Useful for partially erupted molars or anxious children.
Both materials have the same goal: filling the groove. Resin-based sealants generally have better retention; glass ionomer sealants offer the trade-off of fluoride release. The choice depends on the specific tooth and the conditions at placement.
How does a sealant prevent a cavity?
The sealant fills the groove physically. Bacteria cannot settle. No cavity starts.
What does the research show?
~80%
cavity reduction
CDC-cited study: sealants reduced decay in permanent molars by nearly 80% over nine years vs unsealed teeth
72-87%
two-year reduction
2016 Cochrane review of 38 trials: sealed vs unsealed susceptible molars in children
$11.70
averted treatment cost
Per dollar invested in school-based sealant programs, per CDC analysis
The evidence base is among the strongest in preventive dentistry. The 2016 ADA/AAPD clinical practice guideline reviewed 24 studies and concluded that sealants prevent and arrest non-cavitated occlusal carious lesions on the permanent molars of children and adolescents. JADA published the same year reached identical conclusions. NIDCR and CDC reviews are consistent.
Who actually needs sealants?
The simplest rule: deep grooves plus no existing decay. Either the patient has the anatomy that benefits, or they do not. The exam tells us.
Standard recommendation
First permanent molars erupt. The most cavity-prone teeth in the mouth. Seal as soon as the tooth is fully in.
Standard recommendation
Second permanent molars erupt. Same deep groove anatomy. Same recommendation.
Still beneficial
Cavity-free permanent molars at any age remain good candidates. The tooth has not changed; the protection still applies.
Case-by-case
ADA-recognised. Best candidates have no existing decay or fillings on the tooth and elevated cavity risk elsewhere.
Treat first
A sealant over an existing cavity traps bacteria. Restore the cavity, then seal the remaining unrestored grooves if appropriate.
At Serenity Dental, Dr. Husna Khan assesses sealant candidacy at every routine exam for both children and adults. Patients do not need to ask; we flag candidacy as part of the standard preventive workup.
A short clinical aside
Sealants belong to the same broader category of dental procedures as cleanings, fluoride treatments, and routine exams: preventive care. They are not restorative. Restorative dentistry fixes problems that have already occurred. Preventive dentistry avoids those problems from starting. That distinction matters because it changes the conversation about timing, insurance, and clinical priority. Sealants placed at the right moment in a tooth’s life avoid the entire restoration cascade — filling, then larger filling, then crown — that begins when a small groove cavity is missed.
What sealants are not
Sealants are not fillings. They are not whitening. They do not strengthen enamel chemically the way fluoride does. They do not protect smooth surfaces of teeth, only chewing-surface grooves. They are not a substitute for brushing or flossing — the smooth surfaces, the edges between teeth, and the gum line still need regular cleaning. Sealants address one specific decay-prone area.
What should you ask at the appointment?
Three questions cover most patient concerns. Which of my back teeth would actually benefit — a tooth-by-tooth answer based on the exam, not a blanket recommendation. What material will be used and what is in it — a reasonable question worth a clear answer. How long should this last and what should I look for in the meantime — the realistic expectation plus the warning signs.
We answer all three at the appointment without patients needing to prompt. (630) 359-0105 connects to our front desk to schedule.
A short closing thought on terminology
The word sealant tends to mean different things in different contexts. In hardware, sealant is a caulking compound. In construction, it is a waterproofing layer. In dentistry, the meaning is precise — a thin protective resin or glass ionomer coating placed on the chewing surface of a back tooth to fill the deep groove anatomy and prevent cavities. The same word, three different categories of product, three different contexts. The dental version is the one with decades of peer-reviewed research, ADA endorsement, and CDC-cited cavity-prevention data. Confusion about the word is common; the procedure itself is straightforward.
A final practical note
Sealants matter. They prevent cavities in the specific anatomical location where most childhood cavities start, and they do so through a brief, painless, well-evidenced procedure that has been refined across half a century of clinical practice and rigorous peer-reviewed research published in JADA, the Cochrane Library, and CDC-supported epidemiological journals. The procedure takes minutes. The protection lasts years.
Insurance often covers it fully for children. The candidacy bar is low for newly erupted permanent molars at age 6 and age 12, since the deep groove anatomy at those eruption stages is consistently in the range that benefits from sealing — which is exactly why the ADA, AAPD, and CDC all converge on those age windows in their official guidance. Bring the question to the appointment. We answer.
What is a dental sealant -- questions answered
What is a dental sealant?
What is another name for a dental sealant?
How does a dental sealant work?
Are dental sealants the same as fillings?
How long does a dental sealant last?
Who needs dental sealants?
Have dental sealants been used long enough to know they are reliable?
How much does a dental sealant cost?
Educational content only. Recommendations are personalized after an exam and any needed imaging.
About this article
Educational purposes only. ADA, AAPD, CDC, and Cochrane data form the basis of clinical guidance on sealant indications, retention, and safety. Individual results may vary based on clinical findings at your exam.
Related: sealants service page.
Pricing note. Prices shown are approximate Chicago-area 2026 ranges compiled from public cost guides — not a quote or a Serenity Dental fee schedule. Your actual cost depends on your clinical needs, the materials chosen, and your insurance. We provide a written estimate before any treatment begins. Call (630) 359-0105 to confirm pricing for your situation.
Need help with this in real life?
Reading helps. Talking to someone who can look at your actual teeth and symptoms helps more. If you want a clear next step, we’re here.
Related articles
Best At-Home Dental Products: A Bloomingdale Dentist's Honest Guide
A Bloomingdale dentist's honest guide to at-home dental products -- toothbrushes, toothpaste, floss, water flossers, mouthwash, and more.
Read article →Dental Sealants Pros and Cons: Honest Assessment for Adults and Parents
What sealants do well, what they don't, and where the trade-offs are. A direct, no-spin look at the benefits and limits for adults and parents.
Read article →How Often Should Kids Go to the Dentist? A Clear Answer by Age
AAPD recommends every 6 months — but some kids need every 3. What sets the schedule, the age-7 milestone, and what a routine visit covers.
Read article →