Dental Implants
All-on-4 with Bone Loss: Can You Still Qualify Without Bone Grafting?
Most patients with bone loss qualify for All-on-4 without grafting, thanks to angled posterior implants. When grafting is needed and the alternatives.
Written by Dr. Husna Khan, DDS
Serenity Dental of Bloomingdale · April 29, 2026
Educational purposes only. Bone-loss candidacy depends on individual CBCT findings. Call (630) 359-0105 for a complimentary CBCT-guided consultation.
Most patients with bone loss qualify for All-on-4 without bone grafting. The angled posterior-implant design specifically addresses bone-loss anatomy by placing implants where adequate bone still exists, rather than requiring bone at every tooth position. Approximately 80 to 90 percent of patients with moderate bone loss can receive All-on-4 without grafting per published clinical literature. The minority who do need grafting have specific anatomic findings that CBCT imaging identifies before treatment begins.
This guide walks through how bone loss affects implant candidacy, when grafting is and is not needed, what the alternatives are, and how the determination is made at consultation.

Why does bone loss happen before implants?
Three primary causes account for most bone loss seen at consultation.
Tooth extraction without replacement. When a tooth is extracted and not replaced, the bone that previously supported that tooth resorbs because it lacks stimulation. The most rapid bone loss occurs in the first 6 to 12 months — studies cited in AAOMS clinical guidance report 25 to 50 percent volume loss in the first year alone. Patients who lost teeth years or decades ago typically have substantial cumulative resorption.
Long-term denture wear. Conventional removable dentures rest on the gum tissue without stimulating the underlying bone. Patients who have worn dentures for many years typically show progressive bone loss visible on imaging. The 2024 PMC umbrella systematic review on edentulous bone outcomes confirmed that long-term denture wearers lose substantially more facial-skeletal volume than implant-restored patients across decades.
Periodontal disease. Bacterial infection that progresses to bone loss before tooth extraction. Patients who lost teeth specifically because of severe periodontal disease typically have bone-loss patterns that began before the teeth were lost. The disease pattern affects implant planning because remaining bone may be irregular rather than uniformly diminished.
For broader context on what causes implant candidacy concerns, see first All-on-4 consultation and All-on-4 problems and risks.
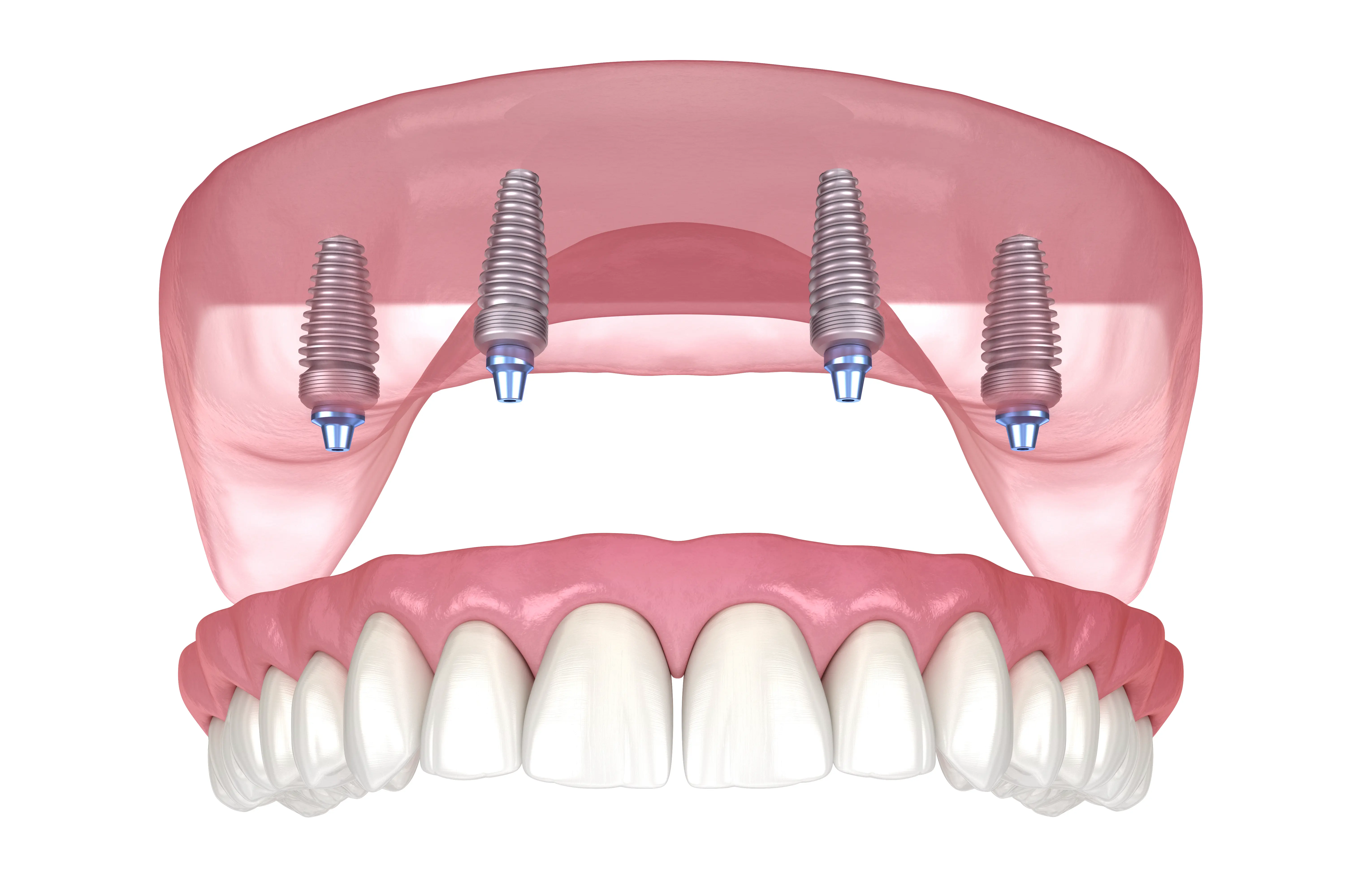
How does the All-on-4 design accommodate bone loss?
The All-on-4 four-implant design is fundamentally different from individual-implant cases that require bone at every tooth position.
Anterior implant placement. The two front implants are placed vertically in the front of the arch where bone tends to be preserved even after tooth loss. The front jaw retains bone better than the posterior because it is denser, less affected by sinus pneumatization, and benefits from continued lip and tongue function.
Angled posterior implants. The two posterior implants are placed at 45 degrees to reach denser bone and avoid the resorbed posterior areas. This design eliminates the need to find adequate bone at the back of the arch — where bone loss is typically most severe in long-term denture wearers and edentulous patients.
Bone-loss tolerance. AAID clinical guidance reports the All-on-4 angled-implant design qualifies approximately 80 to 90 percent of patients with moderate bone loss without bone grafting. The design effectively uses what bone is available rather than requiring rebuilding bone that is not.
Comparison to traditional individual implants. Patients who would need extensive grafting for traditional individual-implant cases (one implant per tooth, 8 to 14 implants per arch) often qualify for All-on-4 without grafting. The cost and timeline savings are substantial when grafting can be avoided.
For the broader procedure framework, see All-on-4 procedure step by step.
When is bone grafting needed?
A minority of cases do require grafting, and CBCT imaging identifies them clearly before treatment.
Severe full-arch resorption. Patients with extensive bone loss across the entire arch — typically long-term denture wearers with 20+ years edentulous — may have insufficient bone even for the angled posterior implants. These cases require ridge augmentation or sinus lift before or alongside implant placement.
Sinus pneumatization in upper-arch cases. The maxillary sinus expands downward into the upper jaw bone after upper-tooth loss. Patients with sinus floor very close to the alveolar ridge may need a sinus lift — elevating the sinus membrane and adding bone graft — to create adequate vertical bone for the posterior implants.
Prior failed implant cases. Patients who have lost previous implants typically have bone defects at the failure sites that may need grafting before re-implantation can succeed.
Specific anatomic challenges. Cleft conditions, prior trauma, or unusual bone anatomy from genetic factors may require grafting to create a normal implant site.
Smoking-related bone changes. Heavy smokers often have additional bone density and quality issues. The 2024 Cureus systematic review confirms smokers have substantially more implant complications. Smoking cessation before grafting and implant placement substantially improves outcomes.
For the broader picture of who is and is not a candidate, see All-on-4 problems risks and regrets.
Bone grafting types and timeline
When grafting is needed, several specific procedures address different bone-loss patterns.
Socket preservation. A small graft placed at the time of tooth extraction to preserve the bone socket for future implant placement. Cost runs $18,000–$30,000 per socket. Heals in 3 to 4 months. Often done alongside extractions if implants are not placed immediately.
Ridge augmentation. A larger graft to rebuild the width or height of the alveolar ridge. Cost runs $18,000–$30,000 per arch depending on extent. Heals in 4 to 6 months before implants can be placed. Used when ridge width or height is inadequate for implant placement.
Sinus lift. Specifically for upper-arch posterior cases where the maxillary sinus has descended into the alveolar bone. The sinus membrane is elevated and bone graft material placed beneath it. Cost runs $18,000–$30,000 per side. Heals in 4 to 6 months for a separate-stage procedure, or implants can sometimes be placed simultaneously for smaller lifts.
Block grafts. Larger autograft blocks taken from another site (chin, jaw, hip) and secured to the recipient site with screws. Used for severe defects. Cost runs $18,000–$30,000 per block. Heals in 4 to 6 months. Less commonly needed with modern materials.
Total timeline. Grafting plus All-on-4 typically runs 6 to 12 months from first consultation to final bridge — compared to the 4 to 6 month timeline for All-on-4 without grafting.
Alternatives when grafting is not feasible
Patients who cannot or prefer not to undergo extensive grafting still have options.
Zygomatic implants for upper-arch cases. Specialized longer implants that anchor in the cheekbone (zygoma) rather than the upper jawbone. Used for cases with severe upper-jaw resorption where conventional implants cannot achieve adequate stability. Specialized procedure typically referred to oral surgeons with specific zygomatic training. Cost runs $18,000–$30,000 per arch.
Implant-supported overdentures with fewer implants. 2 to 3 implants per arch supporting a removable overdenture requires less bone than All-on-4. Cost runs $18,000–$30,000 per arch. Less stable than All-on-4 but works for patients with limited bone or budget. For details see implant-supported dentures guide and All-on-4 vs snap-in dentures.
Phased treatment. Start with simpler treatment that bone allows, then potentially upgrade later. For example, an overdenture initially with implants placed in front-of-arch bone, then conversion to All-on-4 if bone permits over time.
Conventional dentures. Lowest-cost option for patients without adequate bone for any implant approach and unable or unwilling to undergo grafting. Substantial functional limitations compared to implant-based options. For comparison see permanent dentures explained.
What do we tell bone-loss patients at consultation?
Three observations come up consistently when discussing bone-loss cases in our Bloomingdale practice.
The CBCT imaging is more reassuring than patients expect. Patients who arrive expecting to need extensive grafting are often pleasantly surprised that the angled All-on-4 design qualifies them without grafting. The imaging shows exactly where adequate bone exists and lets us plan implant positions with sub-millimeter precision.
When grafting is needed, it is not a setback. Patients sometimes interpret a grafting recommendation as a barrier or failure of candidacy. Modern grafting protocols are reliable, predictable, and well-tolerated. The 3 to 6 month healing extension is real but is not a treatment failure — it is the appropriate biological foundation for long-term implant success.
Long-term smoking cessation matters more for bone-loss cases. Smokers have approximately doubled implant failure rates per the 2024 Cureus systematic review. The effect compounds in patients with bone-loss anatomy where the surgical margins are tighter. Patients who quit before treatment and stay smoke-free have substantially better long-term outcomes.
When should you call rather than wait?
If you have bone loss and are considering All-on-4, schedule a complimentary CBCT-guided consultation rather than waiting or assuming you do not qualify. Many patients are pleasantly surprised at what is feasible without grafting. If you have an existing All-on-4 case and notice loose attachments, persistent gum bleeding, or new pain at any implant — call our office for a prompt evaluation rather than waiting. Schedule an appointment so we can address it before complications develop.
Call (630) 359-0105 for a complimentary CBCT-guided consultation — we determine bone-loss candidacy honestly from your imaging. Related: All-on-4 service page.
All-on-4 with bone loss -- questions answered
Can you get All-on-4 implants with bone loss?
How much bone do you need for All-on-4 dental implants?
Do I need a bone graft for All-on-4?
What if I have severe bone loss?
Is All-on-4 better than bone grafting plus traditional implants?
How long does bone grafting take to heal before implants?
Can bone loss continue after All-on-4?
What causes bone loss before implants?
Educational content only. Recommendations are personalized after an exam and any needed imaging.
About this article
Educational purposes only. Bone-loss candidacy and grafting protocols reflect AAID, AAOMS, AAP, and ADA clinical guidance and 2024 published systematic reviews on full-arch implant outcomes including bone-loss subgroups. Individual treatment selection determined by CBCT-guided planning at consultation.
References
- Article indexed in PubMed Central (PMC), U.S. National Library of Medicine — PMC8015646. pmc.ncbi.nlm.nih.gov/articles/PMC8015646
Related: All-on-4 dental implants.
Pricing note. Prices shown are approximate Chicago-area 2026 ranges compiled from public cost guides — not a quote or a Serenity Dental fee schedule. Your actual cost depends on your clinical needs, the materials chosen, and your insurance. We provide a written estimate before any treatment begins. Call (630) 359-0105 to confirm pricing for your situation.
Need help with this in real life?
Reading helps. Talking to someone who can look at your actual teeth and symptoms helps more. If you want a clear next step, we’re here.
Related articles
Dental Bridge vs Implant: Honest Comparison From a Dentist
Dental bridge vs implant: cost, longevity, healing time, bone preservation, and which is right for your specific case.
Read article →10 Dental Implant Mistakes to Avoid (From a Dentist)
10 common dental implant mistakes that cause failure or regret -- provider selection, planning errors, and post-op care -- and how to avoid each one.
Read article →Dental Implants: Complete Guide for Patients Considering Treatment
Comprehensive dental implants guide -- what they are, how they work, candidacy, procedure, cost, healing, and how to think about implants vs alternatives.
Read article →